This site is dedicated to the
surgical removal of the clitoral hood (prepuce) with the result that the clitoral
glans (the tip of the clitoris) is left permanently exposed. This procedure
(which is sometimes also called "hoodectomy" or "clitoridotomy")
is undergone as elective surgery and its purpose is the enhancement of sexual
response. It is therefore not at all to be confused with clitoridectomy, excision,
infibulation (also known as "Pharaonic circumcision") or any other
form of Female Genital Mutilation (FGM), all of which are generally performed
on non-consenting women or girls and are intended to minimize or eliminate altogether
their enjoyment of sex and all of which are sometimes misleadingly called "female
circumcision"; The Webmaster of this page wholly supports international
efforts to eliminate these forms of FGM.
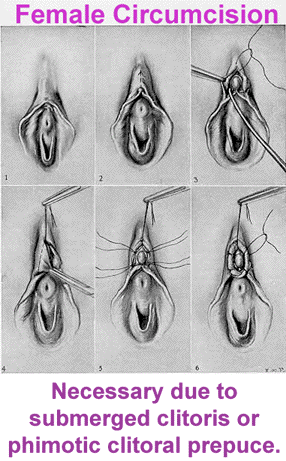
Clitoral Circumcision
Clitoral circumcision: Refers to the surgical procedure in which the hood of the females clitoris (called the clitoral prepuce) is removed. However, the term is often confused in modern day writings with ritual procedures performed in Egypt and in other countries as noted below. On the CIRCLIST website, we refer to female circumcision as only the removal of the hood of the clitoris unless otherwise noted.
Sunna circumcision: Consists of the removal of the tip of the clitoris, sometimes performed by cutting a hole in a piece of cloth and placing it over the area to be cut, limiting the size of the area. In certain cases the clitoris is just nicked with a knife or razor, in parts of Mexico and South America, the sign of the cross is cut into it. Sunna, in Arabic, means "tradition". The clitoral hood is also sometimes removed.
Clitoridectomy: sometimes referred to as excision, which involves the removal of the entire clitoris, rather than just the tip. The labia minora; the inside lips of the vagina are also sometimes removed, but the outer labia are left intact. The vaginal opening is left open and unchanged, rather than sewn together, as in the case of Pharaonic Circumcision.
Pharaonic Circumcision: the entire clitoris is removed, as well as
the inner and outer labia (minora and majora), scraping of the sides of the
vulva and then joining them together and sewing them up with thread or catgut,
or sometimes closing them with thorns. A small opening is left in order that
urine and menstrual blood may pass through. This is also sometimes referred
to as infibulations. A woman who has had this procedure must be cut open to
allow childbirth, and then is re-sewn to ensure faithfulness to her husband.
Female Circumcision: A Factual Bibliography with Annotation
by K. N. Wheeler
I. Personal reports
As far as I know, there have only been two published personal reports (both
by the same woman) by someone who has actually had the surgery. Both were by
Cathrine Kellison, and both were published in Playgirl magazine. The second
article substantially repeats what was published in the first article. Kellison
claims to know several women who had the surgery, and claims that she and all
of these other women have all enjoyed substantial erotic benefits as a result
of the surgery.
Kellison, Cathrine. "Circumcision for Women." Playgirl 1.5
(October, 1973). 76, 124-125.
"$100 Surgery for a Million-Dollar Sex Life." Playgirl 2.12 (May,
1975). 52-55.
II. Medical Studies
To the best of my knowledge, there have been four medical studies of circumcision
of the clitoral hood (prepuce). The earliest report concerns a procedure that
does not actually remove the clitoral prepuce, but stretches it in such a way
as to obtain the result that "It is seldom that the prepuce will overgrow
again once it has been opened." The other three report on results obtained
from the actual surgical removal of the clitoral prepuce. All four report a
striking percentage of those who had the procedure done experience enhanced
sexual enjoyment.
McDonald, C. F. "Circumcision of the Female." General Practitioner
18.3 (September, 1958). 98-99.
(Claims to have circumcised "perhaps 40 patients," including some
adult women. Among the adult women who underwent the procedure, "Very thankful
patients were the reward. For the first time in their lives, sex ambition became
normally satisfied" [98].)
Rathmann, W. G. "Female Circumcision, Indications and a New Technique."
General Practitioner 20.3 (September, 1959). 115-120.
(Sent out a questionnaire to women whose prepuces he had removed, and received
112 replies. Of the 72 women who reported having never experienced an orgasm
prior to the surgery, 9 [12.4%] reported continued failure to achieve orgasm;
64 [87.6%] reported successful achievement of orgasm after the surgery. Of the
39 who reported achieving orgasm only with difficulty prior to the surgery,
5 [12.5%] reported no improvement; 34 [87.5%] reported improvement after the
surgery. Rathmann provides a number of indications and contraindications for
the surgery, and invented a new clamp for the procedure.
Wollman, Leo."Hooded Clitoris: Preliminary Report." The Journal
of the American Society of Psychosomatic Dentistry and Medicine 20.1 (1973),
3-4.
(Provides a "Statistical analysis of one hundred cases." Not clear
whether the statistics Wollman reports include all one hundred women [32 of
whom were not circumcisedösee below] or a statistical report of those who
were circumcised. In this study, he reports the frequency of sexual intercourse
before treatment as 3 times per week on average; after treatment as 5 times
per week on average. 49 women were able to attain orgasm prior to treatment;
92 after. 92 subjectively report improvement in intensity of sexual response,
rapidity of sexual response, and/or greater number of orgasms; 7 subjectively
report no change, and 1 subjectively reports being worse off. The longest time
since treatment was 20 years; 64 patients were followed up after 5 years since
treatment. The treatment occurred in Wollman's office 98 times; in the hospital
[at patient's request] 2 times.)
_______. "Female Circumcision." The Journal of the American
Society of Psychosomatic Dentistry and Medicine 20.4 (1973), 130-131.
(Reports on one hundred consecutive patients referred to him by psychoanalysts
and clinical psychologists. "Sixty eight benefited by surgical female circumcision:
of the remaining thirty-two, twenty-eight showed no need for this procedure;
four refused to be treated by this technique.")
Crist, Takey. "Female Circumcision." Medical Aspects of Human
Sexuality 11.8 (August, 1977), 77.
(Reports on Crist's circumcision of fifteen women, and provides a list of four
conditions for when the surgery would be indicated: "a) they could achieve
orgasm only by masturbation and/or oral sex, b) they could have orgasm in the
lateral or female-superior positions only, c) they stated, "it feels good,
I get there, but suddenly it's over," d) they had a positive cotton-tip
test, where patients felt a distinct difference when a cotton-tipped applicator
was applied directly to the clitoris when the foreskin was retracted as opposed
to application to the foreskin" [77]. Crist's study concludes, "Patients
who have undergone this procedure have generally commented that they have enhanced
sexual response.")
III. Comparison of the Glans of the Clitoris with the Glans of the
Penis
Scott, F. Brantley. "Nerve Endings in Glans Clitoris vs. Glans Penis."
Medical Aspects of Human Sexuality. 15.7 (July, 1981), 88.
(Several argumentsösome, by famous sexologists, such as Masters and Johnsonöhave
been published over the years claiming that the removal of the clitoral hood
should not be compared to the removal of the male foreskin, on the ground that
the clitoral glans was much more sensitive to stimulation than the male glans.
Scott's brief answer to a question sent to the journal would appear to count
against any such claim: "Anatomic studies have shown that on a per centimeter
surface area, the number of nerve endings in the glans clitoris is equal to
that in the same surface area of the glans penis" [88]. The same evidence
would seem to support the surgical removal of the clitoral hood, for women who
find its presence has the effect of dampening stimulation, on the simple ground
that the clitoral glans is so much smaller, and thus offers less opportunity
for stimulation than does the male glans.)
IV. Published Opinions
I do not list these in the bibliography, though several have been published,
because they are generally not supported by either the personal experience of
their authors, or by epidemiological medical studiesöor if such evidence
is cited, the citations are all to the above materials, or else to others' statements
of opinion.
Female Circumcision:
Indications
W.G. Rathmann, M.D.
GP, vol. XX, no. 3, pp 115-120 , September, 1959
Redundancy or phimosis of the female prepuce can prevent proper enjoyment of
sexual relations; yet some modern physicians overlook indications for circumcision.
Indications for, and relative contraindications against, use of this procedure
are presented, and a new technique is described. Properly carried out, circumcision
should bring improvement to 85 to 90 per cent of cases - with resulting cure
of psychosomatic illness and prevention of divorces.
Circumcision of the female is not a new subject. Early writings testify that this problem was known and discussed by physicians of the Roman Empire. Bryk in 1935 compiled a comprehensive book on the history and practice of male and female circumcision. The 265 references abstracted in his text cover the circumcision of the female from the ancient Egyptian era (approximately 1500 B.C.) to the present day. The value of this procedure in improving function has been accepted by various cultures for the past 3,500 years. Although this subject is not new, there are indications for its use that are being overlooked by some modern physicians.
Indications for Circumcision
In general terms, the main indications for circumcision are: (1) functional need - lack of ability to have a climax or ability to have one only with considerable difficulty, (2) an anatomic or mechanical factor that needs correction.
When does this problem present itself and become our concern and responsibility as physicians? It is advisable to investigate sexual compatibility if unexplained symptoms of a psychosomatic type are elicited or if the problem of divorce is present. If there is no shyness or embarrassment on the doctor's part and his attitude is correct, the patient is seldom embarrassed. Often a patient appreciates being questioned on this subject because she had thought this might be her problem. If a patient is not sure that she has ever experienced a climax, it is probable that she has not.
Patients with psychosomatic illness and marital problems make up a good portion of all types of medical practice. If these problems are based on abnormal anatomy, and it is corrected, these patients are often permanently cured. This cure is explained by the common origin of the primitive urges and of the subconscious, from which psychosomatic illnesses develop.
Failure to elicit proper history and to examine patients carefully is illustrated by the following case. Mrs. B. G., age 34, had five divorces before coming to my office as a patient. She was found to have a rather severe redundancy and phimosis, and had never experienced a climax. After being circumcised, she remarried the last man she had divorced and has had no further sexual problem. She stated that she "wasted four perfectly good husbands." While having the five marriages and divorces, she had a great number of psychosomatic symptoms and illnesses. During this time she had been examined and treated by a number of physicians. None of them had told her of the severe phimosis and redundancy or suggested its correction. She has had no recurrence of psychosomatic illness since the circumcision five years ago. No tranquilizers, injections or other treatments were used.
A difficult phase of the problem is presented when the wife of a recurrent ulcer patient states, "What difference does it make that I do not enjoy sex life if I do not refuse my husband"?
In the earlier years of married life this form of prostitution is possibly not too harmful. A number of problems will probably develop in time however, because this practice is contrary to our instincts. If a man is legally married to a woman but not "mated" with her, one of four complications will probably develop: (1) a divorce, (2) another woman, (3) excessive use of alcohol or (4) suppression of normal urges with psychosomatic illness.
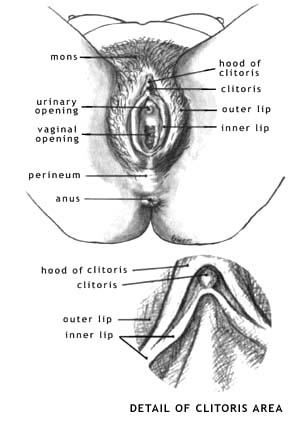
Two Common Abnormalities
The two common problems that make the highly sensitive area of the clitoris unable to be stimulated are phimosis and redundancy. Sebaceous glands about the clitoris attempt to prevent adhesions of the prepuce to it. This sometimes fails and the clitoris is tightly adherent to the prepuce. This defect is recorded as 1 plus or 25 per cent of the normal surface adherent, to 4 plus or complete coverage. A prepuce for the protection of the clitoris is normal and useful, but if it is excessive and extends past the eminence of clitoris it can prevent contact and is harmful. This excess is also classified from 1 to 4 plus. The greatest amount of redundant prepuce I have observed extended approximately one inch past the clitoris so that it is classified 4 plus. Thus, a 1 plus would represent approximately one-fourth inch of redundant tissue. Figure 5 represents a 3 plus redundancy.
In general, the greater the degree of phimosis or redundancy, the greater the probability of satisfactory result by its correction. A 3 or 4 plus phimosis or 3 or 4 plus redundancy could be the anatomic indication. A combination of a 2 plus redundancy and 2 plus phimosis, could be an indication as well. Two rather unusual conditions which could be indications are the hard fibrotic prepuce and the type in which the prepuce is stretched tightly across the glans. Routine circumcision because of a functional problem alone, without the proper anatomic indications, will probably be of no benefit and might be harmful.
Additional Indications
The following situations would indicate the need for circumcision although less phimosis or redundancy is present.
1. If the patient is quite adipose, a circumcision could be indicated although she has less anatomic defect. Obstruction by the adjacent tissues adds to her problem. This operation may help cure her adiposity by relieving psychosomatic factors.
2. If the husband is unusually awkward or difficult to educate, one should at times make the clitoris easier to find.
3. If the clitoris is quite small and is difficult to contact, a circumcision might help by making it more accessible.
Relative Contraindications
On the other hand, there are relative contraindications that make one more cautious and more selective in deciding to operate, for example:
1. Frigidity from psychologic causes, such as fear of pregnancy, early adverse training and experiences.
2. Incorrect attitude of patient or husband concerning desire to be
helped, factors of abnormal jealousy, excessive psychoneurosis.
Labiaplasty is a common request
Physicians have neglected aesthetic surgery of the female external genitalia. However, awareness of female genital aesthetics has increased owing to increased media attention, both from magazines and video. Women may feel self-conscious about the appearance of their labia majora (outer lips) or, more commonly, labia minora (inner lips). The aging female may dislike the descent of her pubic hair and labia. A large pubic fat deposit may be unsightly. Because very few physicians are concerned with the appearance of the female external genitalia, many women seeking help are frustrated. Dr. Alter |
Many women have redundant (long) labia and would like to have them shortened. I know that a surgeon in Canada performs labioplasty. Go to http://www.pulsus.com and click on the Canadian Journal Of Plastic Surgery. Do a search there for labiplasty. I believe the doctor's name is Robert Stubbs. You may also want to go to http:// www.altermd.com

![]()
Article from Scientific American
New scientific evidence favors clitoral hood removal for women with adherent
clitoral hoods
Reports from "Spice
of Life"
"Spice of Life" was a forum for women to talk about sex and sexuality
that shut down in December, 2000. In this archive 76 postings related to the
topic of clitoral hood removal from the "Spice" site are summarized,
including personal reports by 16 different women who had this surgery, plus
8 third-person reports by men and women recalling their knowledge of women who
had undergone this procedure. Although some of those who took part in these
discussions expressed skepticism about the benefits of the surgery, every direct
report from those who had the surgery was strongly favorable regarding enhanced
enjoyment of sex and clitoral stimulation.
Excerpt from item 13 in this document: "I'm happy with my circumcision and haven't seen anything negative about it...any woman who likes sex would benefit from it."
Reports Published in Print Media
Where to Get
the Surgery: Qualified Surgeons
A list of a few clinics where women are known to be able to have this surgery